The body constantly uses glucose. The brain constantly requires extensive amounts of ATP energy, yet unlike other organs, it is unable to use fatty acids as a source of energy. Under regular conditions, the brain is only able to use glucose as its source of energy. The blood transports the needed glucose to the brain.
What methods can be used to maintain a sufficient number of glucose in the blood when nutritional carbohydrates are scarce and glycogen stores are gone, such as during a period of fasting or a low-carb diet? The solution is that certain amino acids can be converted into glucose. Pyruvate can be converted into glucose, but acetate cannot be transformed into glucose. Only acetate is produced when fatty acids are metabolised, meaning glucose cannot be created from fatty acids.
Low-Carb Diets/Starvation
The majority of diets globally have carbs as the main component and glucose normally source from them. When someone does not eat carbohydrates for any purpose, the stored form of glucose, glycogen, is soon gone, forcing the body to generate glucose from amino acids in protein. Over the years, people have typically avoided carbohydrates because they don’t have enough food, which leads to hunger.
During starvation, the body first breaks down the proteins least essential for survival (e.g., some proteins in the liver and skeletal muscle) and, as a last resort, starts breaking down proteins in the heart muscle, etc. Obviously, starvation would be rapidly fatal if the body had to incessantly break down its protein to provide the brain with glucose.
When starvation begins, typically, people have stored fat in their bodies. If the brain had the capability to utilize fatty acids as energy, it could prevent the degradation of bodily proteins and increase endurance. The body produces a fuel substitute derived from fatty acids in response to the lack of glucose, showing that the body thinks it is in a state of starvation.
When glucose is scarce, aerobic metabolism slows down drastically and acetate starts to build up just like when a car on the road stops suddenly and causes all the other cars behind it to stack up. This extraordinary buildup of acetate results in them unifying to make ketones. The brain is able to utilize more and more ketones as a source of energy as it undergoes fasting, reducing the dependence on glucose and lessening the speed of body proteins being broken down. It is certain that if all of the stored fat has been depleted, the body will begin to use its own proteins for energy and will eventually lead to death.
Diets that require reduced intake of carbohydrates are often featured in the plethora of much-used diets for slimming down. They are widely appreciated for their ability to help people slim down rapidly–large amounts of water are eliminated. Glycogen has been used up, and protein is getting broken apart to supply amino acids for the creation of glucose. Glycogen and protein can each absorb up to three times their own mass in liquid, whereas fat is unable to do so. When one has returned to their regular eating habits, the body will quickly replenish the depletions of glycogen, protein, and water, resulting in a noticeable weight gain, which may be a source of disappointment for the dieter.
Weight watchers also enjoy low-carb meal plans as the ketones can lead to decreased hunger, and some of the ketones are expelled from the body through urine and respiration. Ketones possess an energy content, and this “simple burning of calories” is extolled in well-known books endorsing these diets. The amount of energy dissipated is typically no more than 60 calories each day.
Remember that making ketones is a natural reaction to hunger, and in these cases, the advantages of doing so outweigh the possible dangers. The danger with the creation of ketones is the fact that they are acidic, and too much of them can lead to a condition called acidosis or ketosis. This decreases the acidity of the blood and tissue fluid, which can be hazardous to one’s life. It is recommended that you consume 50 grams (200 calories worth) of carbohydrates daily to avoid entering a state of ketosis.
Blood-Glucose
The pancreas produces two hormones, insulin and glucagon, which help control the level of glucose in the blood and keep it within the normal range. When a person consumes carbohydrates, their blood-glucose increases, prompting the secretion of insulin. Insulin creates an environment for glucose to enter cells and for glycogen to be synthesized, thereby decreasing the amount of glucose in the blood. When the body has gone a few hours without food, the amount of glucose in the bloodstream will decrease, triggering the release of glucagon. Glucagon stimulates the liver to convert glycogen into glucose and release it into the bloodstream.
Glycogen is stored in the liver and muscles, but the glycogen in the liver is used to keep blood sugar stable whereas the glycogen in the muscles is to supply glucose for muscle movement.
What is Type 1 diabetes?
Type 1 diabetes is a long-term health issue that is caused by the immune system stopping the pancreas from producing insulin.
Insulin is a key hormone which governs the concentration of glucose (sugar) in the bloodstream. Under normal circumstances, insulin functions in the following steps:
Your body breaks down the food you eat into glucose (sugar), which is your body’s main source of energy.
Glucose enters your bloodstream, which signals your pancreas to release insulin.
Insulin helps glucose in your blood enter your muscle, fat, and liver cells so they can use it for energy or store it for later use.
When glucose enters your cells and the levels in your bloodstream decrease, it signals your pancreas to stop producing insulin.
If the level of insulin in the body is inadequate, an excessive amount of glucose accumulates in the bloodstream, causing high blood sugar which prevents the body from using the nourishment consumed for energy. Neglecting treatment of the situation can result in grave medical issues or fatality. Individuals with Type 1 diabetes must take artificial insulin on a daily basis in order to remain alive and maintain their well-being.
Formerly referred to as juvenile diabetes and insulin-dependent diabetes, Type 1 diabetes is now the accepted terminology.
What is the difference between Type 1 diabetes and Type 2 diabetes?
Both Type 1 and Type 2 diabetes are related illnesses as they are both diabetes mellitus and cause high blood sugar. However, they are not the same condition as diabetes insipidus.
With type 2 diabetes (T2D), the pancreas fails to produce a sufficient quantity of insulin or the body is unable to effectively use the insulin created, usually as a result of insulin resistance. The way one lives their life, including being overweight and not getting enough physical activity, may contribute to the emergence of Type 2 Diabetes in addition to hereditary elements.
In Type 1 diabetes, the pancreas fails to produce insulin. It’s caused by an autoimmune reaction.
Generally, Type 2 diabetes is more common among older individuals, but it is increasingly being seen in kids as well. Type 1 diabetes tends to occur in minors or young adults, but it is something that anyone at any age may suffer from.
Type 2 diabetes is much more widespread than Type 1 diabetes.
Who does Type 1 diabetes affect?
Type 1 diabetes (T1D) can strike anyone, regardless of age, though usually occurring in young children from between 4 to 6 and in the early stages of puberty, which typically falls between 10 to 14 years of age.
Those who identify as non-Hispanic white in the US are the demographic most likely to suffer from Type 1 diabetes, and this condition is almost equally likely to impact males and females.
If you don’t have to have a relative with Type 1 diabetes to acquire the condition, possessing a parent or sibling with Type 1 diabetes increases the possibility of you getting it.
How common is Type 1 diabetes?
Type 1 diabetes is relatively common. There are currently a little over 1.24 million people living with Type 1 diabetes in the USA and it is predicted that this number will increase to 5 million by 2050.
Type 1 diabetes is a frequent and persistent affliction that can occur in people of all ages, most commonly in children in the United States. Though mostly affecting kids, adults may get this diagnosis as well.
What are the symptoms of Type 1 diabetes?
The indications of Type 1 diabetes usually start off mellow and worsen or become more serious over time, which could occur in a spaced out period of a few days, weeks, or months. This is due to your pancreas producing less insulin.
Symptoms of Type 1 diabetes include:
Excessive thirst.
Frequent urination, including frequent full diapers in infants and bedwetting in children.
Excessive hunger.
Unexplained weight loss.
Fatigue.
Blurred vision.
Slow healing of cuts and sores.
Vaginal yeast infections.
It is imperative to consult a healthcare provider and request a Type 1 diabetes test if you or the person under your care experiences any of these symptoms. The sooner you’re diagnosed, the better.
If not treated promptly, Type 1 diabetes can result in a grave situation referred to as diabetes-related ketoacidosis (DKA), making it potentially life-threatening. Seek emergency medical care if you or your child are experiencing any combination of the following symptoms:
Fruity-smelling breath.
Nausea and vomiting.
Abdominal (stomach) pain.
Rapid breathing.
Confusion.
Drowsiness.
Loss of consciousness.
What causes Type 1 diabetes?
Type 1 diabetes occurs when the immune system erroneously assaults and obliterates cells in the pancreas which produce insulin. The harm can manifest itself over a period of some months or even years, leading eventually to a complete absence of insulin.
Although the particular cause of Type 1 diabetes is still unknown, scientists think it is highly likely to be related to genes. The chance that someone will contract the illness if there is no background of the ailment in their family is estimated to be 0.4%. If your mother has Type 1 diabetes, there is a 1-4% chance that you will have it too. If your father has Type 1 diabetes, the likelihood rises to 3-8%. If both of your mom and dad have Type 1 diabetes, then there is a high risk (up to 30%) that you will get it too.
Researchers propose that a virus or hazardous substances in the environment could activate the immune system if an individual is predisposed genetically to Type 1 diabetes, resulting in their body attacking cells in the pancreas.
How is Type 1 diabetes treated?
Individuals who suffer from Type 1 diabetes must make use of manmade insulin on a regular basis – multiple occasions throughout the day – to stay alive and stay fit. They should also make an effort to maintain their glucose level at a healthy level.
There are multiple elements that can alter one’s blood glucose concentration, thus making the management of Type 1 diabetes an intricate and personal task.
Three of the main components of Type 1 diabetes management include:
Insulin.
Blood glucose (sugar) monitoring.
Carbohydrate counting.
Insulin for Type 1 diabetes management
There are several different types of synthetic insulin. Each person begins their laborious duties at varied paces, and the effects remain in their bodies for varying amounts of time. You may need to use more than one type.
Some types of inulin are more expensive than others. Consult with your endocrinologist to determine the best type of insulin for your circumstances.
The amount of insulin you need throughout the day depends on several factors including:
Your weight.
Your age.
Your physical activity level.
The types of food you eat.
Your blood sugar (glucose) level at any given time.
In addition to the regular amount of insulin secretion (usually referred to as the base rate), you will need to inject extra insulin amounts at meal time and to adjust your blood sugar levels when they get too high.
You can take insulin in the following ways:
Multiple daily injections (MDI): Injectable insulin uses a vial and syringe. With each injection, you use a syringe to get the correct dose of insulin out of the vial. You can inject the insulin into the fatty tissue of your belly, upper arm, thigh, or buttocks. Injections are usually the least expensive way to take insulin.
Pen: Insulin pens are similar to injections, but the pen is pre-filled with insulin. Disposable pen needles are usually more convenient than syringes. They can also be a good option for people with low vision.
Pump: Insulin pumps are devices that deliver insulin continuously and on demand. They mimic the way your pancreas would naturally release insulin. Pumps deliver insulin through a tiny catheter (thin, flexible tube) that goes into your belly or another fleshy area of your body.
Rapid-acting inhaled insulin: This type of insulin (known as Afrezza®) is inhaled through your mouth (much like an asthma inhaler). It works much quicker than other types of insulin.
The quantity of insulin you require on a daily basis will fluctuate throughout your life and in specific circumstances. An illustration of this is needing to take bigger portions of insulin during adolescence, conceiving, and while on a course of steroid treatment.
It is essential to consult with an endocrinologist on a continuous basis, usually at least three times a year, to make sure one’s insulin dosages and diabetes control plan are effective.
Blood sugar monitoring for Type 1 diabetes management
Folks with Type 1 diabetes must take great care to check their blood sugar levels regularly all through the day. To stay away from medical problems, keeping blood sugar levels in a healthy range is the ideal choice. You can monitor your blood sugar in the following ways:
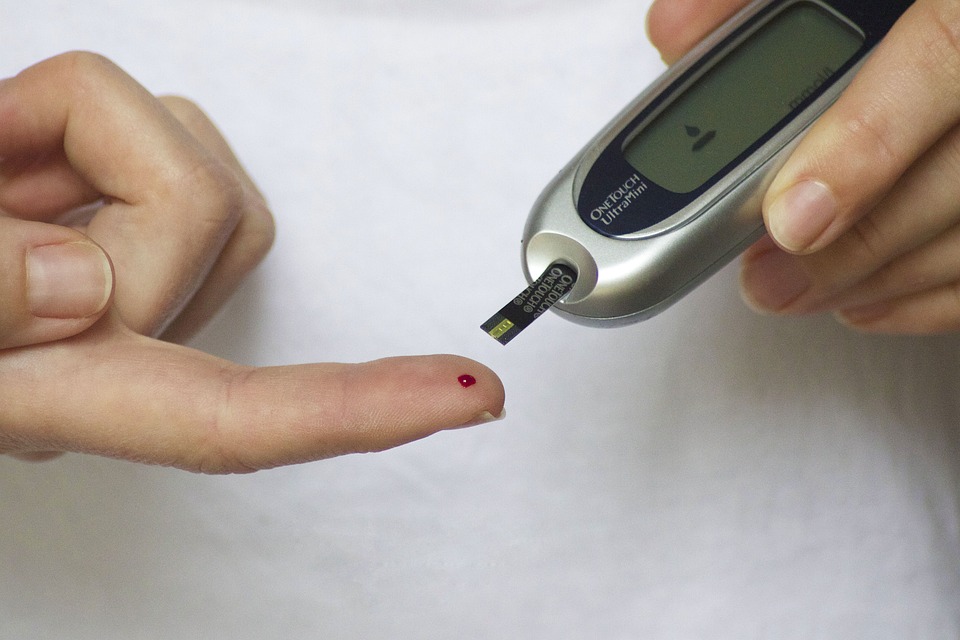
Blood glucose meter: You prick your finger and put a small drop of blood on the meter’s test strip. Your blood glucose level appears on the meter within seconds. A blood glucose meter is usually the least expensive home testing option, but it only reports your blood sugar at the time of the check.
Continuous glucose monitoring (CGM): There are different types of CGMs. Most CGMs require you to insert a small sensor under your skin at home every seven to 14 days. Some CGMs are implanted by a healthcare provider. The sensor continuously records your blood glucose levels. People using a CGM require fewer finger sticks. CGM systems can be more expensive than fingerstick blood glucose meters, but they provide much more information about your glucose levels, including where they have been and where they are going. You can set different alarms to alert you if your blood sugar is trending too low or too high.
Your doctor will advise you of the ideal blood glucose level range you should be aiming for. It depends on a variety of factors, including your: